Compared to other countries in the region, eSwatini has a particularly high prevalence of diabetes and hypertension, with the majority of those affected being undiagnosed. However, the public-sector health system in eSwatini still largely focuses on infectious diseases, and is thus currently ill-equipped to meet the challenges of long-term person-centred chronic care for the large and increasing non-communicable diseases burdens. Like many other countries in SSA, eSwatini provides care for diabetes and hypertension only through physician-led teams in hospitals. Given the severe shortage of physicians in SSA and the low density of hospitals it is clear that major strides in improving secondary prevention of diabetes and hypertension – as well as access to care for other non-communicable
diseases (NCDs) – cannot be achieved unless care for uncomplicated cases of these conditions is decentralised to the primary healthcare system, and thus to nurses and community health workers (CHWs).
The experience of successful large-scale antiretroviral treatment for people living with HIV – which is mostly provided by nurses through public-sector primary care clinics – has encouraged the Swazi Ministry of Health to consider primary care-based approaches for diabetes and hypertension screening, diagnosis, treatment and care. A recent successful feasibility pilot of the World Health Organisation’s Package of Essential NCD Interventions for Primary Health Care in low-resource settings (WHO-PEN) for diabetes and hypertension care in the Lubombo region of eSwatini, has further strengthened the commitment of the Swazi Ministry of Health to establish primary care- and community-based approaches to scale up WHO-PEN for diabetes and hypertension care nation-wide. Using an innovative adaptive national-level randomised controlled study design, our proposed work will generate evidence on the best strategy for scaling up WHO-PEN for diabetes and hypertension to support the Swazi government and policy makers in the wider sub-Saharan region in their policy decisions about the best ‘forms’ of the health systems ‘functions’ required for successful diabetes and hypertension treatment. We will also elucidate factors that enhance and impede the process of scaling up WHO-PEN to generate implementation lessons for other countries in the region. Finally, we will determine whether the scaled-up model maintains (or even improves) its effectiveness over time.
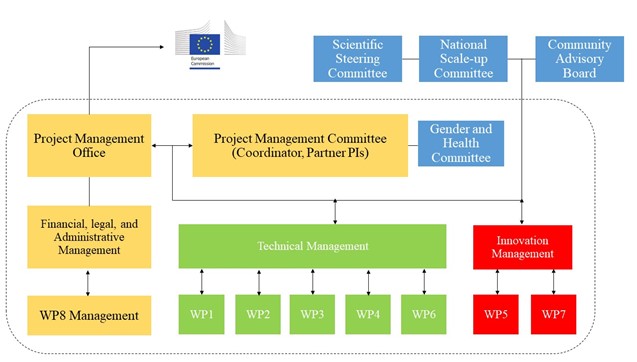
In close collaboration with the Swazi Ministry of Health, our consortium will design, develop and test four novel delivery models to scale up WHO-PEN for diabetes and hypertension to the national level. In this endeavour, we will be supported by three external governance committees, which will be composed of local and global stakeholders and will use two dissemination approaches to facilitate the long-term and broader health and social impact of our project. Figure 1b provides an overview of our governance structure, work focus, and dissemination approaches. The government of eSwatini views this project as the approach to develop a decentralised model for care for non-communicable diseases (NCDs) for long-term national delivery. By establishing rigorous scientific evidence on a national scale-up of a primary care- and community-based NCD delivery models to implement WHO-PEN at scale for diabetes and hypertension care in eSwatini, our work will also provide value to other countries in the sub-Saharan regions, which are planning similar national policy initiatives. Figure 1b: Governance structure, work focus and dissemination approaches
Diabetes and hypertension are a rapidly growing, public health threat in eSwatini. A quarter of Swazis ages 15-69 years old have hypertension and almost one fifth are living with diabetes or pre-diabetes. Diabetes and hypertension and their most deadly complications—cardiovascular diseases (CVD), such as stroke and heart attacks—are responsible for one in five deaths in the country. Of particular concern is that the rate of premature death from these diseases is exceedingly high. The risk of a Swazi hypertensive or diabetic individual dying from their disease before the age of 70 is nearly double that of their counterparts in high-income settings). Moreover, diabetes and hypertension are among the leading drivers of disability in the country, being responsible for the majority of strokes, kidney failure, blindness and lower limb amputation.
NCDs pose a serious public health threat and their prevalence is predicted to rise substantially in the coming years as the HIV epidemic stabilizes and life expectancy increases. Between 2010 and 2015, the number of outpatient consultations for these diseases almost doubled. By 2030, it is predicted that NCDs will kill more Swazis than HIV, TB, malaria and maternal complications. Hypertension and diabetes are already stretching the capacity of the health system to respond. Unless action is taken urgently to reduce the burden of NCDs and their complications, patients with these conditions will overwhelm the physical capacity of health facilities to respond, as well as lead to catastrophic cost burdens that threaten the sustainability of the health system.
Three cross-cutting barriers are identified which prevent those living with hypertension and diabetes from benefiting from the prompt, sustained access to care which could save their lives:
Low detection rate: Lack of systematic screening of high-risk individuals, and lack of diagnostic capacity means that, in eSwatini, 80-90% of diabetics and hypertensives are not aware they have the disease. This means that they cannot take advantage of the protective benefit that lifestyle change and early access to treatment can afford.
Limited access to care: The bulk of NCD care in eSwatini, including screening, diagnosis and routine management, is currently provided by doctor-led teams at a small number of national and regional hospitals. This presents significant structural barriers to access as most of the population lives far from the currently existing hospital facilities as well as economic barriers as patients struggle to afford transportation costs.
Poor disease management: Lack of standardized treatment guidelines for hypertension and diabetes means that quality of disease management is often poor, and varies significantly between facilities and regions. Rolling stock outs of basic medications and diagnostic commodities at the hospital facilities mean that healthcare providers struggle to monitor disease progression and to optimize drug therapy.
Universal Health Coverage (UHC) and the Sustainable Development Goals (SDG) provide a conducive policy environment for guiding the provision of equitable and effective healthcare. UHC is defined as “ensuring that all people can use the promotive, preventive, curative, rehabilitative and palliative health services they need, of sufficient quality to be effective, while also ensuring that the use of these services does not expose the user to financial hardship”. UHC has three related objectives: (1) equity in access to health services, (2) the quality of health services is good enough to improve the health of those receiving services, and (3) financial risk protection – ensuring that the cost of using care does not put people at risk of financial hardship.
SDG #3 is “to ensure healthy lives and promote well-being for all at all ages”. Attached to this goal are 13 specific targets, all of which support the achievement of UHC. Goal 3.4.1 highlights the importance of reducing premature mortality attributed to CVD and diabetes from NCDs through prevention and treatment. The World Health Assembly has adopted a range of global targets aimed at combatting global mortality from NCDs, and accelerating action against the leading risk factors for NCDs and strengthening national health system responses. A mortality target—a 25% reduction in premature mortality from NCDs by 2025 (i.e., the “25 x 25” target)—was adopted by the World Health Assembly in 2013. The world’s leaders have committed themselves to ambitious reductions in premature NCD deaths and is further evidenced in the preparatory processes leading towards the third United Nations High-level Meeting on NCDs, to be held in 2018.
In eSwatini, addressing NCDs will be essential to reach UHC and achieve the SDGs. eSwatini has long recognized the upsurge of diabetes cases and established a national diabetes prevention and control unit in 1999. With the rise of other emerging NCDs, this unit gave birth to a National Prevention and Control of Non-Communicable Diseases Programme. A National NCDs Policy was then developed in response to the need for a comprehensive and cost-effective mechanism to address the growing NCDs in eSwatini. Government considers primary healthcare system strengthening for diabetes and hypertension as a key component of this strategy. As noted in the National NCDs Policy, one of the major government objectives is: “To strengthen and orient health systems to address the prevention and control of NCDs and the underlying social determinants through people-centred primary health care and UHC.”
The current health workforce in eSwatini, however, is insufficient to address NCDs. Moreover, availability and accessibility are a prerequisite for equitable access to services. Acceptability requires having appropriate attributes for the context and work (e.g., gender and age profile of cadres) and health workers need to be responsive and able to provide quality services. This is reflected in the WHO’s recently adopted “Global Strategy on Human Resources for Health: Workforce 2030” which supports both UHC and SDG #3 with the vision to accelerate progress towards UHC and the SDGs. The Workforce 2030 strategy explicitly addresses the issue of improving health workforce performance.
CHWs perform diverse functions related to delivery across the world. While CHWs are usually provided with job-related training, they generally have no formal professional or paraprofessional tertiary education, and can be involved in either paid or voluntary care. The wider use of community-based health workers to provide care and support to people living with chronic health conditions may improve access to care through decentralising prevention, treatment and support to primary and community levels. It may also allow other cadres, such as nurses and doctors, to focus on care for people with more complex problems who need more specialised interventions and may make care more people-centred, as CHWs who come from the same social background as their clients may be able to better understand their needs, especially as these evolve over time with chronic conditions, and communicate effectively with clients. The wider use of CHWs may also help to engage and empower individuals and communities to participate actively in managing their own chronic health conditions and in decisions around the provision of health services. More active self-management is associated with better health outcomes for people living with chronic conditions.
CHWs therefore have the potential to play a critical role in scaling up WHO PEN in eSwatini as well as globally. However, the extent to which CHW programmes for chronic health conditions are able to achieve this goal, and which CHW delivery models are likely to be most effective, feasible and acceptable, needs to be evaluated rigorously. It is important to understand, firstly, whether CHWs can effectively deliver care and support to people living with chronic health conditions, including for which health tasks (such as prevention, disease surveillance, diagnosis, referral for care, treatment and treatment support) and health conditions (diabetes, hypertension, other chronic conditions) they are most effective. Secondly, we need to understand what factors make CHW programmes effective and facilitate their implementation at scale.
A number of systematic reviews have been conducted on the effectiveness of CHWs for different chronic conditions. However, all of these reviews have limitations: firstly, some consider the use of CHWs for specific chronic conditions only – for example, support of people with asthma or cancer screening – or for specific components of chronic illness care – for instance, performing HIV testing. Other reviews are limited by geographic setting considering, for example, studies undertaken in high income countries only. Because these subgroups of the wider population of effectiveness studies on CHWs generally include only small numbers of studies, their results may be misleading. Secondly, many of the reviews do not use robust approaches, such as GRADE to assess the certainty of their findings. This limits the usefulness of their findings for informing decisions. Finally, a number of these reviews are several years old and so do not reflect the full body of knowledge that is available currently. Systematic reviews are also available of the qualitative evidence on CHWs delivering tasks related to chronic health conditions (Vandewalle et al., 2016), but similarly many of these do not encompass all chronic conditions, do not assess how much certainty or confidence can be placed in the review findings, or are out of date.
Finally, a recent systematic review focusing on task-shifting strategies for hypertension and diabetes management suggests that task-shifting is effective but highlights an existing lack of evidence on the widespread implementation of task-shifting strategies (Ogedegbe et al., 2014). The authors of this review concluded that future studies should address implementation as part of existing healthcare systems (WP 2) and their cost-effectiveness (WP 3), both of which are directly addressed by WHO-PEN@Scale.
This project evaluates the scale up of an evidence-based and cost-effective package of NCD services—the World Health Organization Package of Essential Noncommunicable Disease Interventions for Primary Health Care in Low-Resource Settings (WHO-PEN) This package is recommended by WHO as an innovative and action-oriented response to the above challenges in eSwatini. The WHO-PEN package was developed by a multidisciplinary group of international experts in NCDs and is endorsed by members of the Lancet Commission on Diabetes in sub-Saharan Africa, which includes a number of expert members from the WHO-PEN@Scale consortium.
WHO-PEN is a prioritized set of cost-effective interventions that are deemed to be “deliverable to an acceptable quality of care in resource-poor settings” by the WHO. The established cost effectiveness of interventions aims to help to make limited resources go further and the accompanying implementation tools empower nurses and CHWs to more effectively contribute to NCD prevention and care. WHO-PEN is also aligned with the “HEARTS” technical package for CVD management in primary health care, and complements other WHO strategies and packages for population-based primary prevention of CVD, including tobacco control and salt reduction.
Table 1.3b: Selected WHO-PEN interventions
eSwatini has made substantial progress in addressing the HIV epidemic. At the International AIDS Conference in 2017, for instance, it was announced that eSwatini had nearly reached the UNAIDS “90-90-90” targets. It was reported that 87% of people living with HIV were on treatment, and that HIV incidence has decreased by nearly half between 2011 and 2016. This experience of successful large-scale antiretroviral treatment for people living with HIV – which is mostly provided by nurses through public-sector primary care clinics – has encouraged the Swazi Ministry of Health to consider community-based programmes for diabetes and hypertension care. The strong HIV response by the primary healthcare system, in particular, has encouraged government to scale-up the WHO-PEN strategy through nurses and CHWs to improve NCD management.
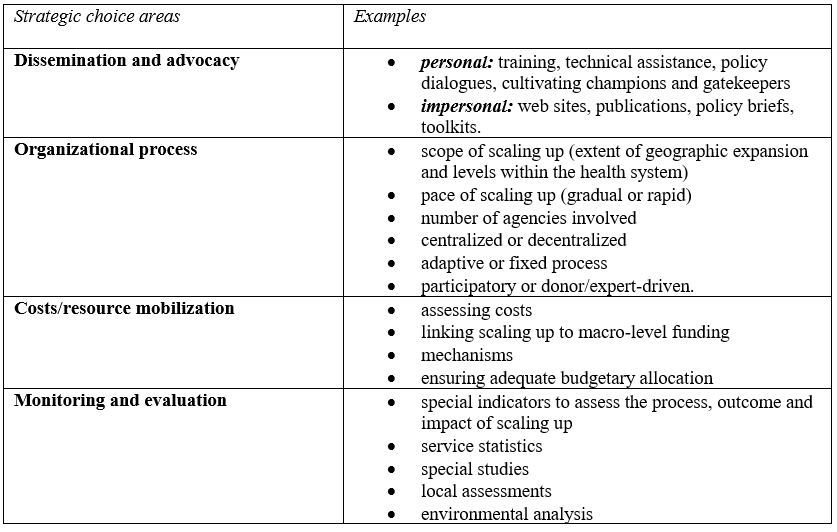
The overall aim of this project is to test four novel community-based programmes for diabetes and hypertension care in eSwatini, by involving nurses and Rural Health Motivators (RHMs) – the government CHW cadre – more actively in healthcare delivery for NCDs in eSwatini. The scale-up of interventions (or their “implementation”–we use the terms interchangeably given the overlap in their definitions) is often considered a complex and incremental process (Pressman J & Wildavsky A, 1984). While WHO-PEN provides clear guidelines on which interventions to scale-up, it is less clear how these should be scaled-up in the context of eSwatini. We conducted a narrative review of the existing implementation science literature on scaling-up task-shifting and included frameworks previously known to the study team. Based on our review, we identified the Framework for Going to Full Scale which provides guidance for large-scale programmes focused on the African region.
The framework consists of the four following steps:
Set-up: prepares the ground for introduction and testing of the intervention
Develop the Scalable Unit, which is an early testing phase
Test of Scale-up, which then tests the intervention in a variety of settings that are likely to represent different contexts that will be encountered at full scale
Go to Full Scale: replicates the intervention in a larger number of sites
The Set-up and the Develop the Scalable Unit phases have been completed in preparation of the scale-up. WHO-PEN@Scale will leverage a feasibility project which was carried out by the eSwatini MoH and other local stakeholders (Communicable Diseases Health Service Delivery (COMDIS), 2017). This pilot study initiated the decentralization of diabetes and hypertension care from the Good Shepherd Hospital to community clinics in the Lubombo region (one out of four regions in eSwatini). The community was mobilized through extensive public engagement around culturally adapt decentralization of NCD care. The 2-year pilot involved 10 intervention clinics and 10 control clinics in Lubombo. The aim was to improve accessibility by providing high-quality NCD care across the region. The pilot study assessed the acceptability, costs, feasibility and effectiveness of adopting WHO-PEN in the public primary care system of eSwatini.
For the pilot study in the Lubombo region, a total of 1,125 patients were recruited to the intervention clinics. 923 (82%) had hypertension alone, 68 (6%) had diabetes alone and 134 (12%) had both diabetes and hypertension. The key results of this feasibility study suggested that overall trends in all health outcomes improved. Medication usage demonstrated that patients were able to change regimes over the intervention with a trend towards combination regimes as recommended by the desk guide. Furthermore, the ability of community clinics to successfully deliver the components of NCD care was demonstrated by process indicators.
The current proposal builds on the major successes and challenges of this pilot to examine national scale up—thereby moving from the “lab” (i.e., the Lubombo pilot) to the “market” (scale-up nationally). Specifically, three key recommendations were developed out of the Lubombo experience that will be leveraged by WHO-PEN@Scale in its evaluation:
WHO-PEN provided by nurses is feasible: we will include shifting care from physicians in hospitals to nurses in primary healthcare facilities in all our intervention arms (WP 2)
Management structures: a scientific steering group, developed during the pilot, has been pro-active in addressing issues and will be included in our project (Section 3.2)
Tools and documentation: training materials were well received and effective during the pilot and will be included here (e.g. desk and training manual) (WP 9)
Considerations for future scale-up at the end of the feasibility study were included in the design of the Lubombo pilot. An action research toolkit was created for this purpose, and for use by others, and was made available through the stakeholders involved with the Lubombo pilot. Nevertheless, before considering any intervention or innovation that has been piloted, it also needs to be confirmed that it is sufficiently robust yet also flexible for application in different contexts for scaling up. The WHO’s CORRECT criteria (defined as Credibility, Observability, Relevance, Relative advantage, Simple enough to install, Compatibility and Testability) were developed for this. The Lubombo pilot has been checked against these criteria, and found to be appropriate for scale-up.
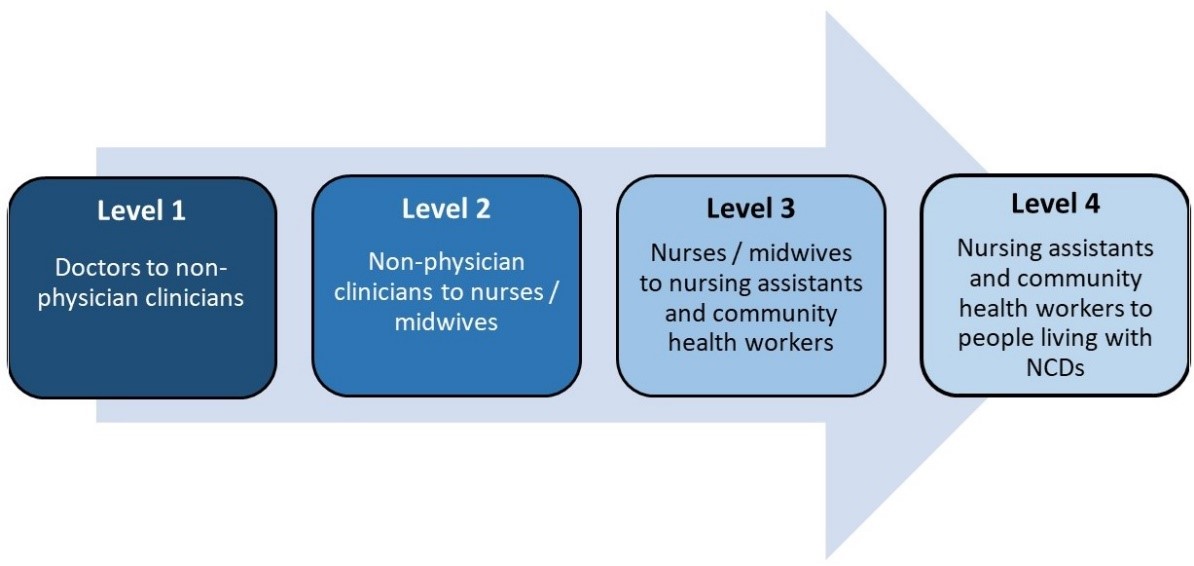
The Test of Scale-up will include feasibility piloting with CHWs. The current proposal will evaluate the scale-up of task shifting both level 2 (non-physician to nurse) and level 3 (from nurse to CHW) as adapted from the global recommendations and WHO guidelines. This phase will take place during an 11-month preparatory period which is built into the project (phase 1 of the randomised controlled trial). We will have the following three aims: (i) to determine the feasibility and cost when WHO-PEN is implemented at large scale, (ii) to determine the impact of WHO-PEN on population health, and (iii) to determine how CHWs can best be employed to improve the delivery of WHO-PEN at scale.
The process of task shifting (WHO)
We hypothesize that task-shifting care to nurses and CHWs will address three existing gaps:
Substantially scale-up detection capacity: CHWs work directly with communities and have been used successfully in eSwatini to increase detection rates for HIV, and to link people with the care they need. Leveraging the expertise and infrastructure developed during the control phase of the HIV epidemic allows for integrated, rapid scale-up of detection capacity.
Sustainably expand access to care for NCDs: most of the eSwatini population lives within 8 km of a clinic. By training nurses to identify, manage and prescribe for these conditions, as well as resourcing clinics with the necessary medications and diagnostic commodities for service delivery, access to care can rapidly and sustainably be scaled-up across the country.
Align care to clearly defined and harmonized standards: by aligning all NCD service delivery around a core set of harmonized interventions (WHO-PEN), care can better be coordinated across all levels of the health system and resource needs per patient, and per facility type, can better be anticipated and planned for.
The next phases (phases 2 and 3) then bring WHO-PEN to Full Scale. We conduct implementation research (WP4) to continuously improve the scale-up of WHO-PEN across eSwatini. We take advantage of the strengths of both quantitative and qualitative methods to complement each other in a sequential explanatory design and allow for a robust analysis. Costing activities will take place for all aspects of the scale-up process. We examine the impact on costs and population health, as well as modelling its long-term cost-effectiveness (WP3). A National Scale-up and Scientific Steering Committee including major stakeholders involved with the scale-up as well as technical experts, will be engaged and meet regularly to further leverage their specific expertise and generate synergies in evaluating the scale-up. Stakeholders involved with the scale-up will also share best practices to ensure that our evaluation is conducted with the highest possible level of efficiency.
In WHO-PEN@Scale, the intervention will be replicated in all four regions of eSwatini (Lubombo, Hhohho, Manzini, and Shiselweni). Therefore, the scale-up is “horizontal”. However, in order to support this, “vertical” scale-up will also need to be facilitated. Vertical scaling up refers to the process of institutionalisation of the innovation with all policy, political, legal, regulatory, budgetary and/or other system changes required. As the process will be country-led, diversification may also occur—particularly in the latter part of the project. There may be proactive leaders at sub-national administrative divisions, e.g. regional level, who might be highly enthused by the innovation and develop the scale-up in their own way. The current project will track all these variations.
We will incorporate the gendered dimension of health in all aspects of WHO-PEN@Scale. From the client’s side, accumulating evidence suggests a reversing disparity in sex disparities in healthcare in Southern Africa. For instance, although HIV care is available to both men and women and nearly free of charge, women are more likely to be tested for HIV, engage in pre-treatment care, initiate treatment earlier, stay on treatment, and survive. Similarly, there is increasing evidence that men needing diabetes and hypertension care are substantially less likely to be diagnosed and to receive appropriate treatment than. Our ASSIST CHW project in eSwatini, however, revealed that CHW coverage among individuals is substantially higher among men vis-à-vis women (adjusted Odds Ratio for female vs. male: 0.59, 95% CI: 0.42–0.83). One important reason for this opportunity to reach men through CHW interventions is that men in eSwatini tend to work in the fields surrounding the house or stay at home when there is no agricultural work be done, while women engage more in market and trading activities outside the. Task shifting to CHWs thus provides an important opportunity through our CHW-component to reach men and to achieve a better gender balance in terms of their health outcomes. We will be sufficiently powered in our analysis to examine our key outcomes differentially by gender (WP2), and we will also focus on the role gender plays in examining the syndemic of NCDs and HIV (WP 5).
From the provider’s side, it is worth noting that most nurses and CHWs in eSwatini are female. In our ASSIST CHW project, however, we found that the lack of balance in gender demographics may have led to suboptimal performance of CHW-led healthcare delivery in. The gender imbalance in the CHW workforce may have led to distrust among patients in CHWs with confidential health information and further impeded counselling success. To achieve better gender balance among these health worker cadres, WHO-PEN@Scale will thrive to increase the participation of men in the CHW training and employment programmes. Our training of nurses at community clinics and CHWs will also be gender-sensitive, building on the gender appropriate training materials developed during the successful Lubombo pilot.
Implementation
This project is implemented through a set of nine WPs.
The table below shows how the WPs interact to produce comprehensive information for policy, which is then effectively disseminated through the activities of WP8 to result in local, regional, and international policy impact. WP9 ensures communication and collaboration across WPs, and monitor timely completion of tasks and milestones.
A Project Management Office (PMO) was set up by the UKHD project manager which represents the consortium in its relations with the European Commission. The project manager runs the PMO and oversees all financial, legal, and administrative management. This includes the production of management products and documents, such as the development of a project website, project templates, and keeping an “issues log” throughout the project. The PMO is also responsible for ensuring good communication amongst stakeholders and the production and dissemination of periodic reports on progress of WHO-PEN@Scale. A consortium agreement was developed, which set out the detailed responsibilities of each partner in the implementation and management of the project as well as monitoring and evaluation arrangements. The overall management structure includes project, technical, and innovation management, as well as advisory bodies (Figure 3.2a).
A Project Management Committee (PMC) was set up comprising the PI from UKHD (chair) and the PIs from each partner. Its roles include: (i) monitoring the implementation of the project—making changes as necessary—and (ii) agreement on annual distribution of research funds. The PMC monitors the implementation of the WPs by each of the WP leads to ensure that they progress according to the agreed work plan set out by the committee. The PMC encourages consortium partners to identify, acknowledge and address any problems as soon as they arise. By including all partner PIs in the PMC, we ensure not only all the key stakeholders are involved in the decision-making process, but also that best practices and expertise can be shared across PIs and WPs. In addition to the regular PMC meetings, collaboration between PIs are further facilitated by supplementary “mini-meetings” dedicated to specific sub-topics. This ensures that data collection and analysis is conducted with a high level of efficiency, allowing us to save valuable resources.
The management of knowledge and innovation is an integral part of WHO-PEN@Scale. We focus on the role and synergies between partners’ experiences, competences, capabilities, and how partners will protect, share, and manage the exploitation of scientific results (WP 8) and intellectual property rights (IPR) resulting from the development of new ICT tools (WP 6). Detailing of the exploitation plans and preparation for innovation activities are continuously followed up throughout the project. A strategy for the knowledge management, protection, and for the exploitation of results was defined for the consortium in the first six months of the project. The strategy is regularly updated during the entire project and periodic reports are submitted to the European Commission.
The PMC meets at least once a year with a Scientific Steering Committee (SSC), an advisory group comprising of external academics and expert observers. Acting Dean Dr. Mosa Moshabela of the School of Public Health, University of KwaZulu-Natal (with expertise in health systems strengthening and controlling chronic infectious diseases in resource-limited settings), and Professor Sally Wyke (as a social scientist who applies social scientific theory and methods to complex interventions to improve health, including gender disparities, in community settings and primary care) have agreed to be in this steering committee. This group will also provide advice on matters related to data safety, management, and responsible conduct of research.
The PMC meets at least once a year with a National Scale-up Committee (NSC). We engage members of regional bodies (e.g., regional office of the WHO), government (e.g., MOH, Ministry of Finance, Ministry of ICT), and expert observers (e.g., NGOs, FBOs). This group advises the consortium about implementation issues locally as well as the communication of scientific results arising from the project.
We engage with the Community Advisory Board (CAB), which functions as a bridge between the local community and the research community. The CAB does not only contribute to the ethical and scientific quality, relevance, and acceptability of proposed research but also encourages community members to be active partners in the development of research in an ongoing, open dialogue with the community, allowing people to express any questions or concerns about the project. We are committed to upholding the ethical and human rights standards of patients and health care workers.
Objectives
The overall objective of the project is to reduce the burden of diabetes and hypertension in Eswatini and the wider sub-Saharan African region. We aim to contribute to the overall objective through the following specific objectives: To
Design and develop two novel community-based programmes for diabetes and hypertension care in Eswatini
Establish the population-level effectiveness and impact of two novel community-based programmes for diabetes and hypertension care in Eswatini
Determine the cost-effectiveness of the preferred community-based programme for diabetes and hypertension care at scale and over time
Develop and implement strategies to tailor community-based programmes to clients with multiple chronic comorbidities (diabetes, hypertension, depression, and HIV)
Develop specific recommendations on the implementation strategy for the scale-up of community-based programmes for diabetes and hypertension care for Eswatini and other countries in sub-Saharan Africa
Synthesize the evidence for different community-based programmes for diabetes and hypertension care at scale
Disseminate evidence on impact and implementation lessons of WHO-PEN@Scale focused on policy makers in sub-Saharan Africa
Role of consortium partners
The WHO-PEN@Scale project is led by the Ministry of Health with support from a consortium of eight institutions from five countries.
It is the main on-the-ground implementing partner for the monitoring, evaluation and data collection activities within the project, specifically; the household surveys, the economic assessments and the qualitative syndemic assessments.
leads on acceptability and implementation activities which include: (1) conducting in-depth interviews with a diversity sub-sample of diabetes and hypertension clients regarding their experiences of the decentralized care model; (2) conducting in-depth interviews with a diversity sample of health care providers implementing the care model; (3) conducting in-depth interviews with Ministry of Health officials/policy makers regarding implementation challenges and bottle-necks and (4) conducting structured observations of the implementation of task-shifting in health facilities.
leads the impact assessment of WHO-PEN@Scale on diabetes and hypertension control and is responsible for the overall management and coordination of the project.
Plan and oversee data collection (implemented by CHAI), and analyze the following components of the WHO-PEN@Scale project: i) bottom-up costing of the WHO-PEN package; ii) questionnaire design and data analysis to ascertain the causal impact of WHO-PEN on household economic outcomes; iii) comprehensive cost effectiveness analysis from the perspective of the Eswatini government; and iv) analyze data from the household surveys to determine the impact of WHO-PEN on health equity.
leads in measuring the syndemic impact of diabetes, hypertension, and HIV at a population level. AIGHD is also tasked with the identification of the main drivers of the syndemics through structural equation modelling. Additionally, AIGHD supports UNESWA in their activities.
It is responsible for the ICT component that will sustainably improve the community health care worker (CHW) counselling process by developing a culturally appropriate and gender-sensitive smartphone app for RHMs.
It has a strong track record of mobilizing support for increased access to services for people living with diabetes and plays a key role in ensuring that project activities are in line with the needs of people living with diabetes.
NIPH will lead WP7, focusing on synthesising global evidence to support the scale up of WHO-PEN, and will co-lead WP8 with CHAI. This work package will focus on engaging with decision makers and other stakeholders and groups to disseminate the findings of the project. NIPH will also contribute to discussions around the other project work packages.
Project Design
This project is an implementation evaluation project, with an innovative two-phase randomized design aimed at informing and evaluating the national scale-up of WHO-PEN for diabetes and hypertension care in Eswatini
The project employs an adaptive randomized design, which allows for i) selection of the most effective community-based programme to deliver diabetes and hypertension care (out of two strategies) after the first phase, and ii) a rigorous assessment of the impact of the most effective community-based programme over a longer time horizon (after the end of the second phase). The randomized controlled study was preceded by a design phase, in which we fine-tuned the approach to implementing the two novel delivery models for WHO-PEN using a rapid prototyping methodology. In both project phases, the project involves one control (Standard of Care) and two treatment arms.
In 2020, the Eswatini government initiated an “emergency decentralization” with the goal to ease pressure on tertiary facilities and to protect people living with diabetes and hypertension because they belong to the high-risk group of COVID-19. As such, care for diabetes and hypertension was shifted from physicians in tertiary facilities to nurses in primary care clinics. Nurses were trained on systematic screening, treatment initiation, lifestyle counselling, and follow-up guided by standardized operating procedures. Clients presenting mild symptoms of diabetes or hypertension are screened whereas those with moderate or severe symptoms are immediately referred to a hospital. Uncomplicated cases are initiated, treated, and followed up by the nurses in the primary care clinics whereas complicated cases are referred to tertiary facilities. Prescriptions are given to the client on a monthly basis.
In the Differentiated Service Delivery (DSD) model arm, three existing DSD models, which were originally developed for HIV care, were adapted for non-communicable disease (NCD) care: The facility-based fast track model, the facility-based treatment club model and the community-based adherence groups. The eligibility criteria for the DSD models are detailed in Table 1 and the client can choose which model they prefer to be enrolled in depending on their specific needs. Participation is voluntary and clients can decide to not opt in. In the fast track model, clients are given three-month prescriptions or drug refills (depending on drug availability) and an appointment for their next medication collection. Both reduce the transport costs and waiting time a client has to spend for obtaining NCD care. When a client arrives at the clinic, they receive preferential treatment and undergo basic health checks, such as tuberculosis (TB) screening. If no health concerns arise, the client collects their medication from a designated fast-track dispensing point at the facility. As semi-annual health check-ups are required for clients with hypertension or diabetes, each fast-track visit is followed by a normal clinic visit three months later where the client will be treated according to the treatment guidelines described under the standard of care. After these regular visits, the client will be given a three-month drug prescription/refill and a date for the next fast track appointment. The second facility-based DSD model, facility treatment clubs, are groups of a maximum of 20 clients with hypertension and/or diabetes. During the bi-monthly meetings at the facility, the facilitator (usually a nurse) provides general health counselling on diabetes, hypertension, nutrition, physical exercise, HIV, and cervical and prostate cancer screening. Furthermore, the weight of all participants is recorded and clients receive medication/prescriptions for the next two months. Every six months, the clients receive a full health check-up at the clinic after the club meeting. If a client is unwell during any of the meetings, they are referred either to the clinic or a tertiary facility for an immediate check-up. The third model, community-based adherence groups, are groups of a maximum of six clients with hypertension and/or diabetes who meet monthly in their respective communities. Groups are composed of members of an existing social network such as family members, friends, or colleagues. They are equipped with a blood pressure monitor and a point of care glucometer to monitor their blood pressure/glucose during each meeting. Members are trained on the use of these devices, recording results in their client cards, as well as on screening each other for symptoms of TB and referral procedures. Team members take turns in collecting the medication for the entire group from the clinic, thus saving time and money through cost sharing. This ensures that clients receive the recommended health check-up at least every six months and obtain their medication without having to visit the clinic every month. Each group has a nurse who can be contacted in case of challenges and questions. This model primarily targets clients living in remote, hard-to-reach areas. Clients enrolled in either DSD model are advised to visit the health facility anytime they feel unwell, not to wait for the next appointment.
The second treatment arm, the community distribution point (CDP) arm, leverages existing community outreach sessions that offer HIV care and will extend their services for clients with hypertension and/or diabetes. CDPs are sites that are set up temporarily within a community once a month in central locations such as community centres or schools. Each CDP is linked to one clinic, which means that CDPs are organized through this clinic. A team consisting of nurse and additional health personnel offers NCD screening, treatment initiation for hypertension, adherence support, and counselling according to the standardized treatment guidelines. Complicated cases will be referred to tertiary facilities. Diabetes treatment initiation is doctor led, therefore clients will be referred to doctor led healthcare facilities. Clients will receive monthly drug refills for both hypertension and diabetes, depending on NCD drug availability at the respective CDP site. When there are stock outs nurses will prepare a prescription sheet for clients to purchase drugs at nearby pharmacies.
Both treatment arms additionally involve the government-led and funded community health worker cadre, the Rural Health Motivators (RHMs). The RHM Programme is a community-based health care volunteers programme, which was established in 1976 by the Eswatini Ministry of Health to facilitate the extension of health promotion services to the communities through interpersonal communication. They currently offer services focused on basic health promotion messaging for sexual and reproductive health, nutrition, and child health. To ensure participation and ownership of the community, RHMs are chosen by traditional community leaders and trained by the Ministry of Health. There are over 3,000 RHMs covering the entire country and every household should be visited by an RHM at least once a month. RHMs are a non-salaried and non-specialist cadre. The majority of RHMs is between 40 to 50 years old and over 90% is female.
In WHO-PEN@Scale, RHMs are involved with the following tasks: i) basic screening of clients at risk of diabetes and/or hypertension ii) extensive, personalized lifestyle counselling, iii) referral of clients at risk of diabetes and/or hypertension, and iv) monitoring treatment adherence and health status of clients with diabetes and/or hypertension, v) demand creation for services offered in the respective treatment arm. RHMs screen clients based on their age, sex, and waist circumference. They are equipped with standardized guidelines on screening as well as health messaging. In the DSD arm, RHMs will refer clients to clinics and in the CDP arm to the CDP site. In both treatment arms, urgent cases will immediately be referred to clinics or tertiary facilities.
Results coming soon ...
Results
I am text block. Click edit button to change this text. Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
1
75%
2
90%
3
80%
4
80%
Results
Lorem ipsum dolor sit amet, consectetur adipiscing elit.
Graphic 1
R1
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Graphic 2
R2
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Graphic 3
R3
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.